



US funding cuts to IPPF’s partner in Sudan, the Sudan Family Planning Association (SFPA), have impacted the delivery of essential SRH information, services and training in a time of civil war.
Background: a historic and strategic partner
Sudan’s civil war has created one of the world’s largest humanitarian crises, with 13.4 million refugees, asylum-seekers and internally displaced persons[1]. Maternal mortality is high at 256 deaths per 100,000 live births, gender-based violence is rampant in displacement camps, and health infrastructure has been severely degraded[2]. In this context, SRH services are about survival. Against this backdrop, the sudden withdrawal of international funding sets Sudan up for catastrophe.
For sixty years, SFPA has served as a critical pillar of the nation’s health system, working in close partnership with the Federal and State Ministries of Health to provide maternal and child health and SRH services. Today, however, that mission is being tested by a conflict that reached its 1,000th day in January 2026. WHO reports that over a third of health facilities nationwide are now non-functional due to physical damage, a lack of basic supplies, and deadly attacks on medical staff, leaving millions of people in a desperate struggle for health assistance[3]. Despite these immense challenges, SFPA keeps going, working across 14 of Sudan’s 18 States through a network of clinics, mobile teams, and community midwives. Continuation of SFPA’s services has never been needed more.

Impact: the strain on the health system
While SFPA does not receive direct funding from USAID, it does receive funding from partners such as UNFPA, WHO and the Global Fund, which have faced significant budget reductions in 2025. With UNFPA funding support, SFPA provides SRH services across 12 States and GBV services across 7 States. Funding cuts passed on by UNFPA to SFPA in 2025 led to reduced frequency of SFPA’s community outreach activities, with some teams operating for only 4-5 months instead of 12. As other service delivery organisations have had to close down, the burden on SFPA has grown.
While SFPA struggles to meet the demand, donors and partners are working tirelessly to support the public sector to restore and revive health services across the country. In 2025, UNFPA and WHO supported SFPA to rehabilitate and equip multiple public sector hospitals, including maternity hospitals, and primary health centres, and funding for Emergency Obstetric Care teams.
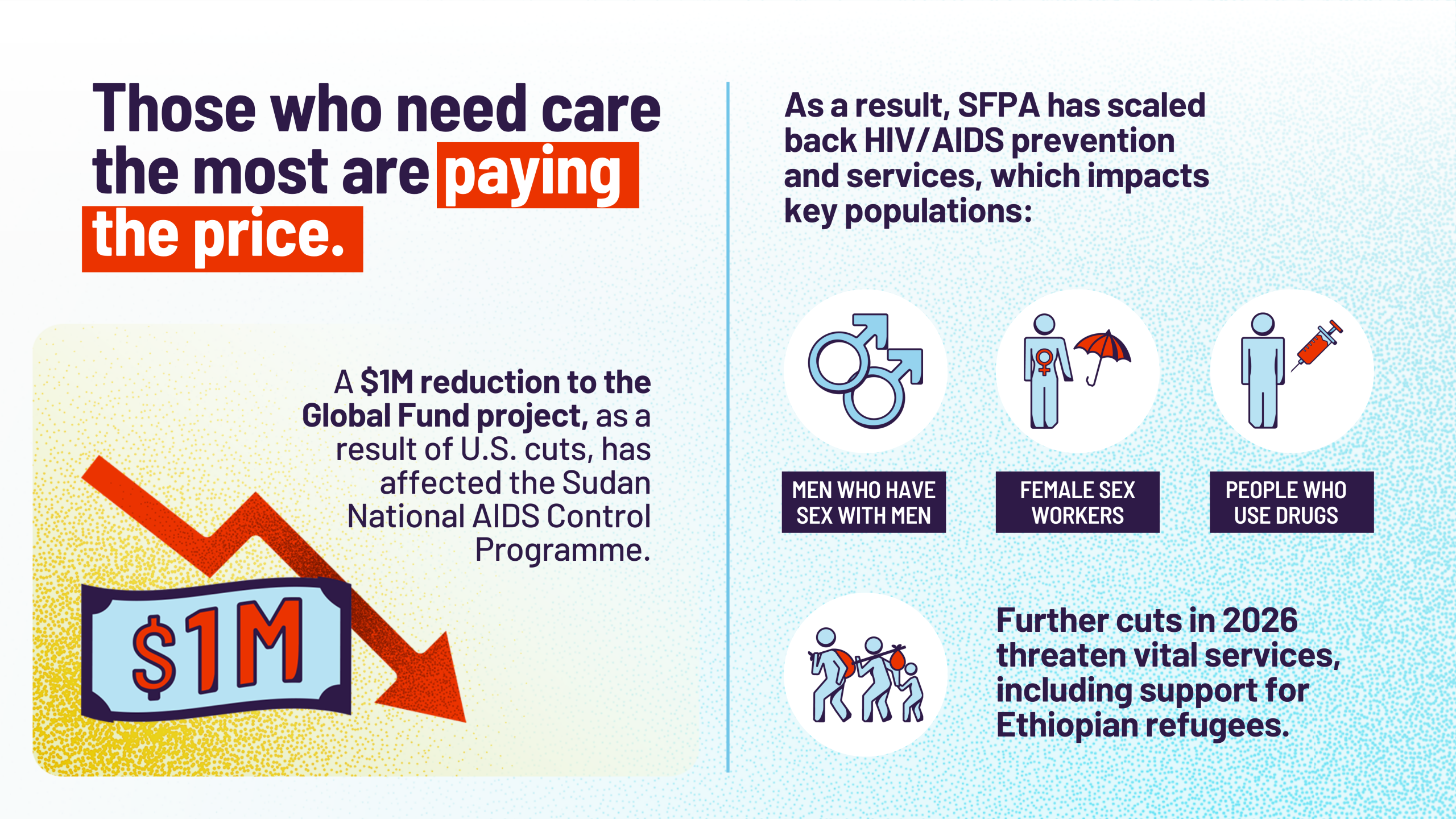
SFPA reports that the Sudan National AIDS Control Programme has also been affected due to a $1 million cut to the Global Fund project as a result of US cuts. Subsequently, SFPA’s work providing HIV/AIDS prevention and services to key populations (men who have sex with men, female sex workers, and IDUs) has been reduced. SFPA fears that further budget reductions in 2026 will hinder their continued support to these vital facilities, services and populations, including Ethiopian refugees with who they have been working with since 2020.
{kind=link}
This crisis extends beyond daily care to the very future of Sudan’s health workforce. Since the war began in 2023, midwifery schools have been closed due to insecurity and a lack of resources. UNFPA had funded SFPA to pilot the national task shifting policy by training public sector medical assistants and midwives to be able to administer long-acting contraceptive methods and to provide clinical management of rape. This has now become part of the national training programme, where UNFPA supports SFPA to train in-service midwives, provide refresher and on-the-job training, and supportive supervision. SFPA reported that in 2025 however, due to funding cuts, they were only able to conduct ten in-service training sessions with the support of UNFPA – a fraction of the numbers of trainings in prior years. Funding reductions mean fewer trainings can be conducted and limits SFPA’s ability to support public sector midwives.
Adapting for 2026 and beyond
SFPA is bracing itself not just for further funding cuts but also for continuing to operate in an unstable and unsafe environment. To mitigate these volatile risks, the team is expanding its fundraising capacity, focusing on broadening the range of income-generating services offered at their facilities to include paediatrics, community pharmacies, and nursery daycare, and expanding their digital health interventions such as telemedicine. However, these adaptations are likely marginal compared to the scale of existing, and growing, need. Without a renewed commitment from the international community, reaching people across Sudan with vital, life-saving SRH services will be increasingly difficult.
{kind=link}
Conclusion
The experiences shared by IPPF MAs and CPs demonstrate that the withdrawal of US funding has not only reduced budgets. It has also dismantled vital service delivery infrastructure, severed lifelines for millions of people – particularly the most marginalised and excluded – and exacerbated the triple threat of financial cuts, political volatility and anti-rights movements. From the immediate, devastating operational contraction — including staff layoffs, clinic closures, and contraceptive insecurity— to the indirect but significant service disruption via cuts to partner agencies, the human cost of this geopolitical realignment is catastrophic.
Amidst this systemic failure, IPPF’s Harm Mitigation Fund has been a critical lifeline, preventing total organisational failure and providing the necessary breathing room for MAs / CPs to survive the immediate shock. However, this emergency support has only partly stabilised a precarious situation, not restored pre-crisis capacity. The future of SRHR now hinges on the ability of MAs/CPs to pivot towards new, resilient operating models: a stronger focus on domestic financing, the rapid expansion of social enterprise models to subsidise care for the most vulnerable, and active diversification of funding streams.
Ultimately, the present crisis demands more than just damage control. It necessitates the urgent construction of a new, sustainable global architecture for SRHR. The dedication and resilience shown by MAs in the face of these challenges is undeniable. Their path forward, however, requires committed support for financial sustainability, continued advocacy to hold governments accountable, and a unified global effort to ensure that the fundamental human right to sexual and reproductive health is upheld.
[1]United Nations High Commissioner for Refugees (2025). 2025 Mid-Year Trends Report. https://www.unhcr.org/sites/default/files/2025-11/mid-year-trends-report-2025.pdf
[2] World Health Organization (2025). WHO Global Health Observatory. https://data.who.int/indicators/i/C071DCB/AC597B
[3] WHO press release: Sudan: 1000 days of war deepen the world’s worst health and humanitarian crisis